Immunosuppression: why and how?
Background:
Care is taken to perform compatible transplants by checking antibodies to blood (ABO) and tissue (HLA) antigens.The rejection of transplanted organs is caused by the activation of lymphocytes. HLA class 1 molecules are present on all nucleated cells and help the immune system to distinguish self from non-self. HLA class 2 molecules are only present on antigen presenting cells (dendritic cells, monocytes, macrophages). The dendritic cells of the donor tissue migrate to the recipients lymphoid tissue and present them to the recipients lymphocytes, activating the overwhelming armamentarium of of the immune system.
Once activated, the T lymphocytes differentiate into cytotoxic T cells, tumor suppressor cells, and T-helper cells; The B lymphocytes become plasma cells and memory cells.
There are essentially two types of rejection although a mixed pattern can be seen:
1. cell mediated rejection due to T-lymphocytes
2. antibody mediated rejection due to by B- lymphocytes.
Care is taken to perform compatible transplants by checking antibodies to blood (ABO) and tissue (HLA) antigens.The rejection of transplanted organs is caused by the activation of lymphocytes. HLA class 1 molecules are present on all nucleated cells and help the immune system to distinguish self from non-self. HLA class 2 molecules are only present on antigen presenting cells (dendritic cells, monocytes, macrophages). The dendritic cells of the donor tissue migrate to the recipients lymphoid tissue and present them to the recipients lymphocytes, activating the overwhelming armamentarium of of the immune system.
 |
| All blood cells arise from a common stem cell but the lymphocytes follow a different lineage. |
There are essentially two types of rejection although a mixed pattern can be seen:
1. cell mediated rejection due to T-lymphocytes
2. antibody mediated rejection due to by B- lymphocytes.
Immunosuppression strategies: risks, induction, maintenance.
These have evolved over the last 50 years as our understanding of the immune system has improved. The exact regimen is based on the recipient’s immunological risk for rejection, infection and malignancy. A balanced approach is required because aiming for zero rejection will result in the patient succumbing to overwhelming infections or malignancy.
These have evolved over the last 50 years as our understanding of the immune system has improved. The exact regimen is based on the recipient’s immunological risk for rejection, infection and malignancy. A balanced approach is required because aiming for zero rejection will result in the patient succumbing to overwhelming infections or malignancy.
Induction immunosuppression is given at the time of transplant to quickly subdue lymphocytes. This is comprised of high dose solumdrol in combination with either:
- lymphocyte blocker: Simulect (Basiliximab)
- lymphocyte killer: Campath or thymoglobulin.
Maintenance immunosuppression regimens include the following medications.
- calcineuin inhibitor: Tacrolimus (prograf, Envarsus) or cyclosporin (Neoral)
- antiprolifertaive: myfortic, cellcept, azathioprine
- steroid: prednisone
- mTor inhibitor: Everolimus, sirolimus.
- Co-stimulation blocker: Belatacept (Nulojix)
Immunosuppression therapy is based on the transplant recipient’s immunological risk and comorbidities.
1. Low immunologic risk
This group consists of first-time transplant recipients who have less than 20% panel-reactive antibodies and no donor specific antibodies. The induction is typically with basiliximab, and they are maintained on a calcineurin inhibitor in combination with an anitproliferative agent. Steroids are not used long term.
2. Intermediate immunologic risk
This group consists of transplant recipients with panel-reactive antibodies between 20% and 80% and no donor specific antibodies. They are induced with basiliximab and maintained on a triple drug regimen. Intermediate immunologic risk recipients receive induction with simulect and are maintained on a calcineurin inhibitor, mycophenolate, and prednisone. A steroid free regimen may be appropriate if Campath or Thymoglobulin is used to induction.
3. High immunologic risk
This group consists of transplant recipients who have rejected one or more transplants aggressively (i.e. within the first year post transplantation), or any recipients with greater than 80% panel-reactive antibodies. Transplant candidates receive lytic induction with Campath or Thymoglobulin. They are maintained on a calcineurin inhibitor (cyclosporine or tacrolimus), prednisone, and mycophenolate mofetil.
Other considerations:
mTOR inhibitors:
These drugs (Zortress, Rapamune) are useful if the recipient has a history of malignancy, the graft has scarring or if the calcineurin dose needs to be reduced. They are not used routinely because of significant side effects such as poor wound healing, hyperlipidemia, mouth ulceration, and proteinuria.
NULOJIX for longterm maintenance instead of calcineurin inhibitors.
 |
| The Nulojix molecule blocking second signal needed for T cell activation. |
Nulojix is a co-stimulation blocker that prevents activation of lymphocytes. The calcineurin inhibitors act within the lymphocyte after the cell has already been activated. After the initial loading period, it is given every 4 weeks as a 30 min infusion. Patients that are at lower immunologic risk and have difficulty taking medications correctly are very good candidates for this. Follow up studies to 7 years was published int he NEJM that showed better patient and graft survival when compared to calcineurin inhibitor.
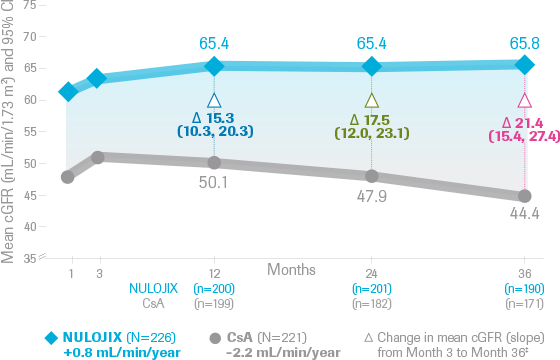 |
| Patients on Nulojix have better kidney kidney function long term. |
Our program has evolved over time as our experience with Nulojix has grown. Any patient that is EBV positive and not high immunologic risk is a good candidate for starting with Nulojix. It is also a very good choice in those that tolerate calcineurin inhibitors poorly or have difficulty remembering to take medications correctly.

Comments
Post a Comment